
Why dental MRI is suddenly on every dental radiologist’s radar
For the past three decades, dental MRI has been talked about as the imaging modality of the future — radiation-free, superb for soft tissue, but too slow, too noisy and too poor at bone to replace a CBCT or an OPG in day-to-day practice. That picture is now changing fast.
Between 2024 and 2026, three things have happened in parallel. First, black bone MRI sequences have matured to the point where cortical bone can be measured on MRI to within roughly 1 mm of CT. Second, dental dedicated MRI (ddMRI) scanners — purpose-built, lower-field machines with dedicated intraoral and mandibular coils — have been validated in clinical trials and, as of March 2026, cleared by the FDA. Third, dental MRI protocols have been shown, in peer-reviewed prospective studies, to be accurate enough for guided implant surgery in carefully selected patients.
None of this means CBCT is going away. But if you refer dental and maxillofacial imaging, it is worth understanding exactly what dMRI can and cannot do in 2026, when it is a genuine alternative to a CBCT scan, and where it is likely to sit alongside cone beam in the next five years. This guide is written for dentists, endodontists, periodontists, orthodontists, oral surgeons and maxillofacial consultants who want the evidence-based version, not the marketing version.

What is dental MRI (dMRI)?
Dental MRI, often abbreviated dMRI, is the application of magnetic resonance imaging to the dentomaxillofacial region using specialised pulse sequences, dedicated receive coils and optimised protocols that compensate for the small anatomy, restoration-related artefacts and motion challenges unique to the oral cavity.
Unlike a standard head MRI, a dental MRI uses one or more of the following:
- Dedicated surface coils, including 15-channel mandibular coils that conform to the jaw and inductively coupled intraoral coils that sit close to the tooth of interest, both of which substantially improve signal-to-noise ratio over a generic head coil.
- Specific sequences — high-resolution 3D T1-weighted turbo spin echo, T2-weighted STIR (short-tau inversion recovery), 3D double-echo steady-state (DESS), and low flip-angle gradient-echo “black bone” sequences — chosen to balance hard tissue visualisation, inflammation detection and artefact suppression.
- Isotropic sub-millimetre voxels, typically around 0.4 mm, allowing multiplanar reconstruction comparable in-plane to a CBCT volume.
- Field strengths from 1.5T through 3T for conventional systems, and increasingly low-field (0.55T) dental-dedicated platforms designed for in-practice use.
The result is a three-dimensional dataset that shows cortical and cancellous bone, tooth pulp, periodontal ligament, inferior alveolar nerve, muscles of mastication, salivary glands and mucosal soft tissues — without ionising radiation.
dMRI vs CBCT: the honest comparison
For clinicians used to referring for a cone beam CT, the key question is simple: when is dental MRI a better choice, and when is CBCT still the right answer?
Where CBCT wins
CBCT remains the reference standard for most hard-tissue dentomaxillofacial tasks. It is faster (typically under 30 seconds of acquisition), cheaper, more widely available, and gives unambiguous submillimetre cortical and trabecular bone detail. CBCT is the imaging of choice for:
- Routine implant planning and surgical guide fabrication
- Complex endodontic diagnosis — missed canals, resorption, fractures, periapical lesions — where it is particularly valuable (see our dedicated article on why every dentist should use Morita CBCT for complex endodontic and root canal treatment)
- Pre-surgical planning for impacted third molars, cysts and benign jaw lesions
- Sinus assessment prior to lift procedures
- Structured radiology reporting for medico-legal and multidisciplinary use
Where dental MRI wins
Dental MRI pulls ahead when the diagnostic question turns on soft tissue, inflammation, or repeat imaging of radiosensitive patients. In 2025, a prospective study in patients with severe periodontitis showed that dMRI reliably detected infrabony and furcation bone loss, and — more importantly — picked up bone marrow oedema and inflammation in tissues that looked structurally intact on CBCT, producing what the authors called a “mismatch lesion pattern” closely associated with active disease. No CBCT can show you that, because inflammation itself has no CBCT signature.
The same advantages apply to:
- Pulp vitality and pulpitis — dMRI can quantify pulp signal changes and differentiate vital from non-vital pulp tissue, an area reviewed in depth in a 2025 Journal of Magnetic Resonance Imaging paper.
- Inferior alveolar nerve tracing before third molar surgery or implant placement, where direct visualisation of the nerve (rather than inference from the canal) is a genuine advantage.
- Oral soft-tissue tumours and vascular malformations, where distinguishing a haemangioma from an irritation fibroma pre-operatively can prevent serious intraoperative bleeding.
- TMJ assessment — although CBCT is excellent for the osseous components of the TMJ, MRI remains the gold standard for the disc, retrodiscal tissues and joint effusion, and a combined CBCT + MRI workup is often the highest-yield strategy in complex TMD.
- Paediatric and radiosensitive patients, where even the comparatively low dose of a CBCT is worth avoiding if an equivalent diagnosis can be made without radiation.
The evidence on accuracy
For implant planning, a prospective in-vivo study of 45 implants in 30 patients found that dental MRI-based treatment plans showed excellent inter-rater and inter-modality agreement with CBCT, with mean three-dimensional deviations of 1.1 mm at the entry point and 1.3 mm at the apex, and a mean angular deviation of 2.4°. All but one of the surgical guides derived from MRI alone were suitable for clinical use. A 2025 systematic review and meta-analysis from Sheffield concluded that although MRI showed a slightly greater deviation in implant tip placement of around 0.3 mm, its overall accuracy was comparable to CBCT.
For cortical mandibular bone, a 2025 study from MD Anderson comparing black bone MRI with CT in head and neck cancer patients found agreement within ±0.85 mm — clinically acceptable for monitoring early osteoradionecrosis without cumulative radiation exposure.
The honest bottom line: for most implant cases today, CBCT remains the pragmatic choice and the reference standard. For inflammation-driven periodontitis monitoring, pulp assessment, nerve visualisation and repeat paediatric imaging, dMRI is already a defensible first-line or adjunct modality in specialist hands.
Black bone MRI: the sequence that changed the conversation
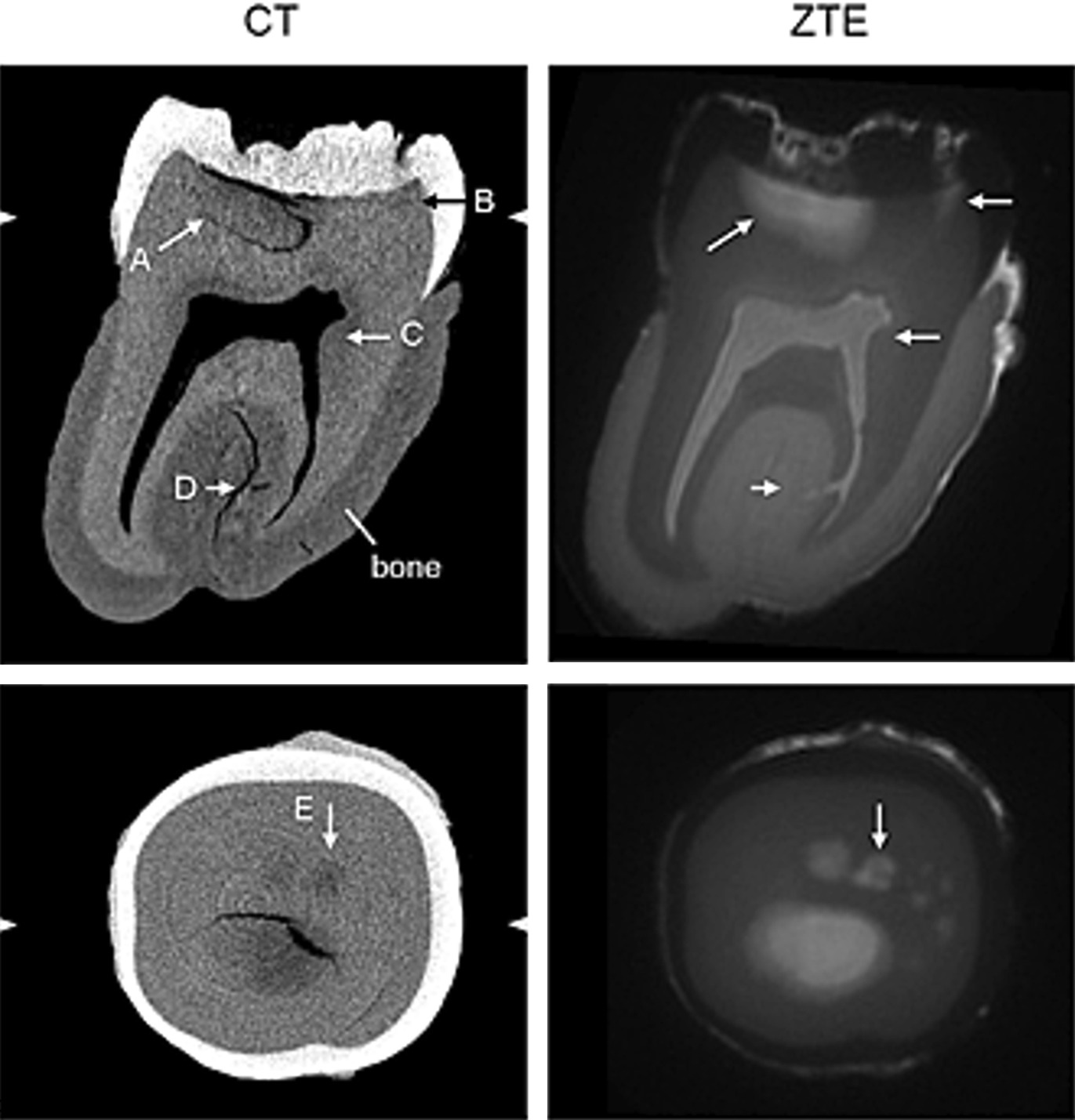
Most clinicians know MRI “can’t image bone”. That is not quite true. Cortical bone has almost no free water protons, so it returns essentially no MR signal — but that very absence can be exploited. Black bone MRI, first published by Eley and colleagues in Oxford, uses a low flip-angle (around 5°) gradient-echo sequence with a short TR and TE that suppresses both fat and water signal uniformly. The result is soft tissue that appears uniformly grey and cortical bone that appears uniformly dark — a high-contrast image that can be segmented and 3D-reconstructed to produce CT-like renderings of the craniofacial skeleton.
The 2025 Journal of Clinical Imaging Science systematic review of black bone MRI in clinical practice concluded that the technique now offers a reliable, non-ionising alternative for craniofacial assessment, with particular value in paediatric and radiation-sensitive populations. Clinical applications already validated include:
- Diagnosis of craniosynostosis in infants, with 3D reconstruction quality approaching CT
- Delineation of fracture-prone regions in oral and maxillofacial trauma (2025 Zurich/Maastricht study)
- Monitoring of cortical mandibular thinning and early osteoradionecrosis after head and neck radiotherapy
- Assessment of buccal bone thickness for immediate anterior implant planning — a 2023 pilot showed 3D-DESS MRI produced confidential diagnostic accuracy for bone thickness compared with CBCT
Limitations matter. Black bone MRI struggles at air-bone interfaces such as the paranasal sinuses, where “black bone” abuts “black air”. Dental amalgam, orthodontic brackets and titanium implants still produce susceptibility artefacts. And the scan remains longer, louder, claustrophobic for some patients, and far more costly per study than a CBCT.

Dental dedicated MRI (ddMRI): the scanner built for dentistry
Until recently, every dental MRI was performed on a general-purpose hospital scanner, which is why access has been limited and costs high. That is starting to change.
In January 2024, Greiser and colleagues published the technical specifications and feasibility of a dental-dedicated MRI (ddMRI) system in Dentomaxillofacial Radiology: a low-field scanner with a dedicated radiofrequency coil optimised for the dentomaxillofacial area and tailored pulse sequences, explicitly designed to lower the barriers to MRI adoption in dentistry.
On 9 March 2026, Siemens Healthineers and Dentsply Sirona announced the MAGNETOM Free.Max Dental Edition — described as the first-ever dental-dedicated MRI — had completed clinical validation and received FDA clearance. The clinical evaluation report highlighted the scanner’s ability to differentiate active inflammation from scar tissue, support non-invasive pulp vitality assessment, and visualise teeth and nerves together in a single acquisition. A parallel NIH-registered clinical trial asks a blunter question: can ddMRI replace low-dose CBCT in routine dental practice? Data from that study are due in 2026.
Whether ddMRI becomes a fixture in UK specialist practice over the next three to five years will depend on capital cost, throughput, reimbursement and how the General Dental Council and the faculties respond. For now, the relevant point for referrers is that purpose-built dental MRI is no longer theoretical.
Practical indications where dMRI changes management today
Translating the evidence into clinical practice in 2026, dental MRI — whether on a conventional 1.5T/3T system with a dedicated coil, or on an emerging ddMRI platform — is worth considering in the following situations:
Endodontics. Ambiguous pulpitis, suspected internal resorption where CBCT is equivocal, or a tooth being considered for vital pulp therapy in a young patient where repeat imaging over months is anticipated. For the full CBCT perspective, see our overview of CBCT in endodontics.
Periodontology. Severe periodontitis with apparent clinical-radiographic mismatch, monitoring response to regenerative therapy, or identifying active inflammation beyond the bony defect. dMRI is not yet a replacement for clinical attachment level measurement or bitewings, but it adds a biological dimension.
Implant dentistry. Patients who are pregnant, paediatric, or undergoing staged treatment over several years where cumulative dose is a concern. Also patients with straightforward partially edentulous spaces where MRI-derived guides have been shown to be accurate to within a clinically acceptable margin. Complex cases and full-arch work still belong on CBCT.
Oral and maxillofacial surgery. Pre-operative mapping of oral soft-tissue lesions, characterisation of vascular malformations, suspected perineural invasion, and follow-up of benign tumours. See our CBCT in ENT and maxillofacial page for the complementary hard-tissue workflow.
Orthodontics. Cephalometric analysis without ionising radiation is feasible on MRI, and there is emerging literature on MRI-based cephalometric tracing in children, though a conventional ceph X-ray remains the pragmatic standard.
TMJ disorders. Always MRI for the disc, CBCT for the condyle and eminence. In difficult TMDs both are often needed.
Limitations you should brief your patients on
Dental MRI is not a drop-in replacement for a 15-second panoramic X-ray. Honest limitations include:
- Scan time: typically 10–20 minutes versus under a minute for CBCT or an OPG. Motion artefacts matter.
- Claustrophobia: a real and common reason for non-completion on conventional closed-bore scanners.
- Metal artefacts: amalgam, crowns, orthodontic wires and existing implants all degrade the image in predictable ways.
- Contraindications: pacemakers, non-MRI-conditional implanted devices, certain aneurysm clips, and retained ferromagnetic foreign bodies.
- Cost and access: a private dental MRI is considerably more expensive than a CBCT, and the number of UK centres offering truly dentally-optimised MRI protocols remains small.
- Reporting expertise: dMRI requires a radiologist familiar with both dentomaxillofacial anatomy and MRI physics. At 3Beam, our radiology reports are produced by specialists led by Dr Rebecca Davies, currently focused on CBCT; dMRI reporting should follow the same principle of specialist interpretation.
What this means for referrers in 2026
If you are a dentist, endodontist or maxillofacial surgeon in London, the practical takeaway is this. For 95% of your day-to-day hard-tissue imaging questions — missed canals, implant planning, third molar assessment, periapical pathology, sinus evaluation, TMJ bony architecture — a well-performed, properly reported CBCT remains faster, cheaper and at least as accurate as any MRI currently available. A same-day CBCT at 3Beam with a next-day structured report from a specialist radiologist is hard to beat for routine work.
For the remaining 5% — the inflammation-driven, the soft-tissue-dominated, the paediatric, the repeat-imaging cases — dental MRI is now a real option rather than an academic one. Over the next three to five years, as dental-dedicated MRI scanners come to market and reimbursement catches up, expect that proportion to grow.
For the majority of referrers, the right posture in 2026 is to keep referring for CBCT and OPG as your first-line 3D imaging, to know which questions dMRI answers better, and to build a working relationship with a radiologist who can advise on the cases at the margin. You can always discuss a complex case with us directly — see our for referrers page, or use the contact form for a same-day reply.
Frequently asked questions
Is dental MRI the same as a head MRI? No. A dental MRI uses dedicated surface or intraoral coils, sub-millimetre isotropic voxels, and sequences tailored to the jaw — black bone, STIR, DESS and 3D T1 turbo spin echo. A standard head MRI has neither the resolution nor the artefact-handling to answer most dental questions.
Does dental MRI use ionising radiation? No. MRI uses magnetic fields and radiofrequency pulses. It is the main reason dMRI is being developed as a complement to CBCT for paediatric, pregnant and serially imaged patients.
Can dental MRI replace CBCT for implant planning? In research settings, MRI-based surgical guides have been shown to be clinically acceptable for straightforward cases, with sub-1.5 mm deviations at the implant apex. In routine UK practice, CBCT remains the reference standard, and a pragmatic dental CT scan is still the right first-line investigation for almost all implant cases.
What is black bone MRI? A low flip-angle gradient-echo MRI sequence that makes cortical bone appear uniformly dark against grey soft tissues, allowing CT-like 3D reconstruction of the facial skeleton without ionising radiation. Its main current applications are craniofacial, paediatric, trauma and oncology follow-up imaging.
What is dental dedicated MRI (ddMRI)? A new class of lower-field MRI scanner, of which the Siemens MAGNETOM Free.Max Dental Edition became the first FDA-cleared example in March 2026, purpose-built for dentomaxillofacial imaging with specialised coils and sequences and designed for in-practice or near-practice installation.
Does 3Beam offer dental MRI? 3Beam is an independent diagnostic imaging centre at 86 Harley Street specialising in CBCT, OPG, cephalometric and DEXA imaging. We do not currently operate an MRI scanner on site. For most dental and maxillofacial imaging questions, our same-day CBCT service is the most pragmatic option. For cases where dMRI is clearly indicated, we are happy to discuss the referral pathway with you.
Further reading on 3Beam
- Structured dental CBCT radiology reports: clinical standards and applications
- The cutting-edge role of CBCT in TMJ assessment
- Why every dentist should use Morita CBCT for complex endodontic and root canal treatment
- OPG dental X-rays: precision panoramic imaging for better diagnosis
- Dental CT scan cost (UK): what you’ll typically pay
3Beam is an independent CBCT and dental radiology centre at 86 Harley Street, London W1G 7HP, providing same-day scanning and specialist radiology reporting to dentists, maxillofacial surgeons, ENT consultants and chiropractors. To refer a patient or discuss a complex imaging question, register as a referrer or call 0207 637 8227.