
CBCT scans and reports at 86 Harley Street
Introduction: This guide is designed to help dentists systematically interpret CBCT scans in endodontics. CBCT technology provides high-resolution, three-dimensional imaging that is invaluable for assessing root canal morphology, periapical pathology, and treatment outcomes. Proper interpretation is essential to ensure accurate diagnoses and optimal patient care. A structured and detailed approach can improve consistency and enhance clinical decision-making.
Step 1: Understanding When to Use CBCT in Endodontics
Before reviewing a CBCT scan, consider the clinical indications:
- Identifying complex root canal anatomy: Useful for detecting additional canals, unusual curvatures, and anatomical variations such as C-shaped canals.
- Detecting periapical pathology: Helps distinguish between periapical cysts, granulomas, and abscesses by assessing lesion borders, internal structures, and effect on surrounding bone.
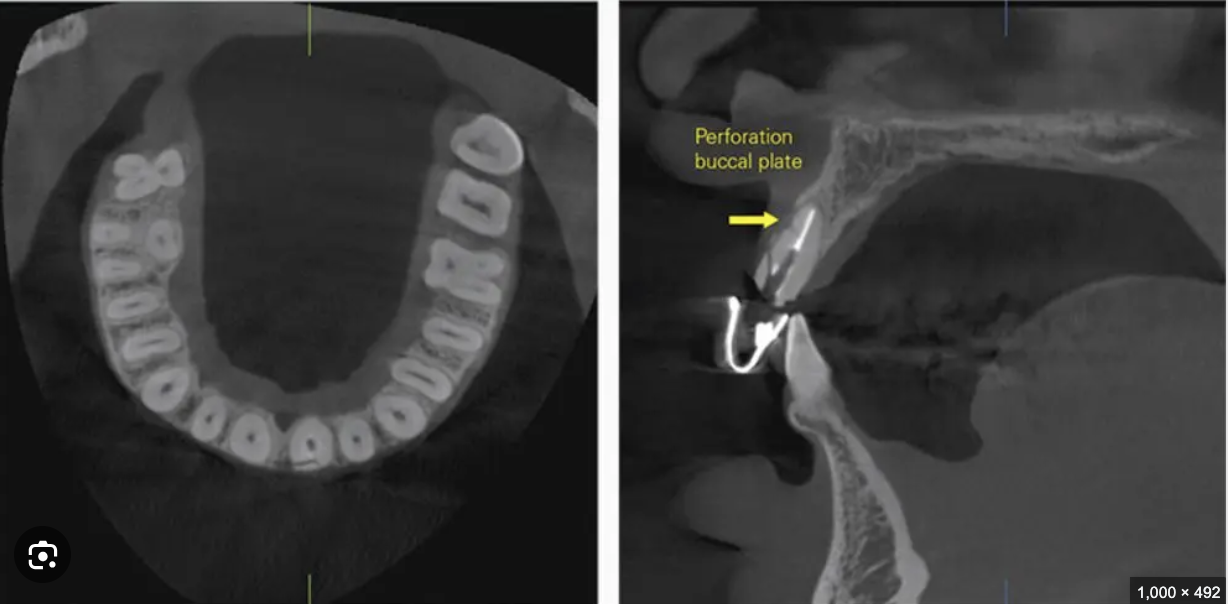
- Assessing treatment complications: Essential for detecting vertical root fractures, root perforations, and endodontic failures that may not be visible in conventional 2D radiographs.
- Evaluating post-treatment healing: Assists in monitoring bone healing, changes in periapical radiolucencies, and detecting persistent infections.
A thorough patient history, clinical examination, and justification for CBCT imaging should guide its use, in accordance with ALARA (As Low As Reasonably Achievable) principles.
Step 2: Checking Image Quality and Orientation
Before analysis, ensure the scan is of diagnostic quality:
- Confirm proper orientation: Ensure axial, coronal, and sagittal views are correctly aligned to avoid misinterpretation.
- Adjust contrast and brightness: Optimising window settings can enhance visibility of fine details, particularly in the periapical region.
- Identify any artefacts: Recognise beam-hardening, motion, or metal artefacts that may obscure diagnostic structures and adjust accordingly.
Step 3: Systematic Review of the Scan
To ensure no key details are overlooked, follow a structured approach:
a) Root Canal System
- Identify root canal morphology, including variations such as extra canals, isthmuses, and curvatures.
- Look for calcifications or obstructions that may impact treatment.
- Assess previously treated canals for signs of underfilling, overfilling, or unfilled spaces that may harbour bacteria.
b) Periapical Region
- Evaluate periapical radiolucencies for size, shape, and margin definition.
- Differentiate between acute and chronic periapical lesions by examining bone changes and lesion demarcation.
- Look for cortical bone perforation, which may indicate an aggressive or expanding lesion.
c) Cortical Bone and Trabecular Patterns
- Detect signs of sclerosis, bone resorption, or periapical rarefaction.
- Assess cortical plate integrity and possible expansion in the presence of pathology.
- Identify any trabecular changes suggestive of infection, metabolic bone disease, or systemic conditions affecting bone density.
d) Surrounding Structures
- Examine the proximity of root apices to the maxillary sinus, mandibular canal, and mental foramen.
- Look for sinus membrane thickening, which may indicate odontogenic sinusitis.
- Identify neurovascular structures to avoid iatrogenic complications during treatment.
Step 4: Recognising Common Endodontic Pathologies
- Periapical Lesions: Differentiate between cysts (well-defined corticated border), granulomas (diffuse non-corticated border), and abscesses (ill-defined with potential sinus tract formation).
- Root Fractures and Resorption:
- Vertical root fractures: Look for radiolucent lines extending through the root structure, often accompanied by lateral radiolucency.
- External resorption: Identify irregular root surface defects, particularly in cases of trauma, orthodontic movement, or inflammation.
- Internal resorption: Observe symmetrical enlargement of the root canal with well-defined margins.
- Missed or Untreated Canals: Detect untreated canal spaces or accessory canals, which can contribute to persistent infection and treatment failure.
- Perforations: Assess for iatrogenic perforations, their location, and their impact on periapical bone.
Step 5: Writing a Structured CBCT Report
A well-documented report should include:
- Patient Information and Clinical Indication: Clearly state the reason for CBCT acquisition and relevant history.
- Scan Quality and Limitations: Note any artefacts or limitations that may affect diagnostic accuracy.
- Findings (structured by region): Provide a detailed description of anatomical and pathological findings.
- Impressions and Recommendations: Offer a concise summary and suggest appropriate next steps, including treatment planning or referral to a specialist if needed.
View our sample CBCT report from 3Beam Imaging Centre.
Step 6: Legal and Ethical Considerations
- Documentation: Ensure that all findings are accurately recorded in the patient’s records, along with justifications for CBCT use.
- Referral: Consult an oral and maxillofacial radiologist when uncertain about findings, particularly for non-endodontic pathology.
- Informed Consent: Obtain patient consent before performing CBCT imaging, ensuring they understand radiation exposure and clinical benefits.
- ALARA Principle: Use CBCT only when conventional radiographs are insufficient for diagnosis.
Conclusion
Using a structured and detailed approach to CBCT interpretation enhances diagnostic accuracy and improves patient outcomes. A thorough understanding of endodontic anatomy, pathology, and radiological principles is essential for correct diagnosis and treatment planning. By following these steps, dentists can confidently analyse CBCT scans and ensure clinically relevant findings are properly documented and communicated.
This guide serves as a comprehensive reference for everyday clinical practice, reinforcing the role of CBCT in modern endodontics and ensuring high standards of patient care.
3Beam Imaging Centre provides high-quality CBCT reports prepared by UK-based, GDC-registered dental radiologists, under the leadership of Dr Rebecca Davies – ORDER YOUR CONE BEAM CT REPORT HERE
CBCT radiology reports cost £130 for any size field of view with a turnaround time of 5 working days, and with 24-hour turnaround available as express.